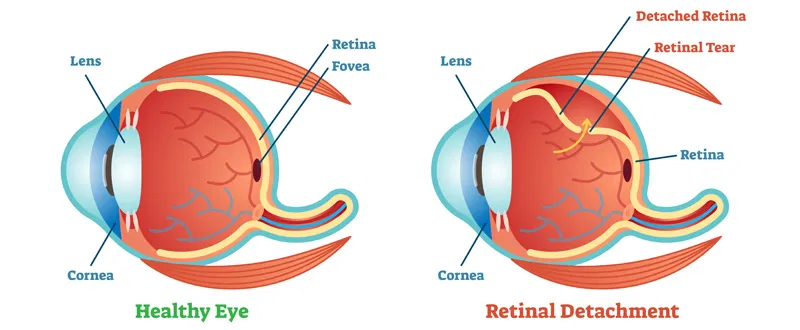
What Is Retinal Detachment?
Many people think that if they have 20/20 vision, they have perfect vision. This is not true. The 20/20 value is just a comparison. An eye with 20/20 vision can see at 20 feet the same things that a “Normal eye” can see at 20 feet. Some people can see even better than that. They may be able to see at 20 feet what a ‘normal eye’ would only see at 15 feet; that is 20/15 vision. Know more about 20/20 vision in this article.
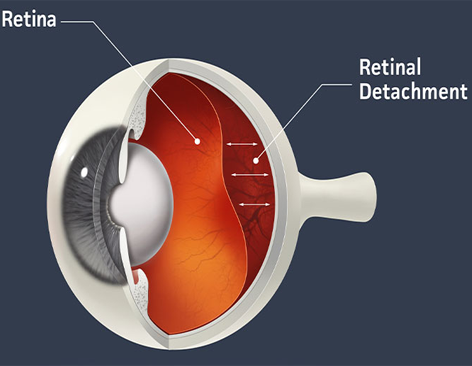
How Does Retinal Detachment Occur?
What Would Be the Symptoms?
How to Diagnose Retinal Detachment?
How to Treat a Retinal Detachment?
Surgical Repair: The repair of retinal detachment may be approached by 3 different methods.
1. Pneumatic Retinopexy: In a select group of cases, one may successfully attach the detached retina by injecting a gas bubble in the eye, treating the retinal hole with freezing (Cryo) or laser and positioning the eye to enable successful closure of the hole. This is the simplest of the treatment approaches with least intervention. The success of this procedure is about 70 per cent and in case of failure, the next procedure can be done with improved success (up to 90 per cent).
2. Scleral Buckling: Most simple retinal detachments are handled by applying a silicone buckle on surface of the eye, thus indenting the walls inside. The retinal hole is treated with freezing (Cryo) and the fluid that has collected between retine and underlying layers is usually removed. The success of this surgery is usually very high, with almost 90 per cent of eyes having retinal reattachment with one procedure.
3. Viteoretinal Procedures: For more complex retinal detachments, complicated surgery called vitreoretinal surgery is needed. In this, the diseased vitrous is removed along with abnormal scar tissue. The retina is attached by use of air, gas or silicone oil. The success of these surgeries varies with type of case. Sometimes, multiple surgeries may be indicated in case of recurrences. Where silicone oil is used, it is usually removed after variable period of time, once the retina is successfully reattached. The final success can be declared only if retina remains attached after removal of silicone oil. Obviously the more complex will be the surgical procedure needed and less will be the cure rate.
It is important to understand that surgical success and visual recovery need to go hand in hand. The visual recovery depends upon the basic strength in the retina, the duration of retinal detachment and most importantly the health of the central, most importantly the health of the central, most sensitive part of the retina called the macula. Reading fine print needs excellent vision, hence only a percentage of the eyes with complex retinal detachment can regain reading capabilities. More often, mobile vision is retrieved. Failed surgery usually leads to non recovery of vision and on occasions these eyes may shrink.
The surgery may be done under local or general anaesthesia, where gas/air silicone oil is injected the surgeon may advocate special posture. With gas in the eye, air travel is restricted Eye drops or ointment may have to be instilled for 6-8 weeks and glasses are prescribed at final examination. With simple buckling surgery, vision may start recovering in a few days time, but final vision is known after 6 weeks. With more complex vitreo-retinal surgeries, it takes longer time for visions to improve and stabilize.
In Summary
Patients with symptoms of retinal detachment require prompt attention by an ophthalmologist who will thoroughly examine the interior of the eye and advise about the need for treatment.